
Dissociative Identity Disorder (DID): All You Need to Know
Introduction
Dissociative Identity Disorder (DID), previously known as Multiple Personality Disorder or split personality disorder, is a complex psychological condition primarily caused by severe trauma during early childhood. This trauma often involves extreme, repetitive physical, sexual, or emotional abuse. Understanding the intricacies of DID is crucial for effective diagnosis and treatment, which can significantly enhance the quality of life for those affected. This article delves into the history, challenges, and recent advancements in diagnosing and treating DID, aiming to dispel myths and highlight the importance of a multidisciplinary approach.
History and Evolution of Dissociative Identity Disorder ( DID)
The history of Dissociative Identity Disorder (DID) reveals a complex evolution of understanding, marked by early cases and shifting diagnostic perspectives.
Early Accounts of Dissociative Identity Disorder ( DID)
- The first documented case resembling DID dates back to 1584 with Jeanne Fery, whose detailed records of exorcism described symptoms consistent with DID, including multiple alters with distinct identities and abilities. Her case, involving trauma from severe abuse, was later highlighted by Bourneville in 1886 as a quintessential example of the disorder.
- In 1623, Sister Benedetta’s case involved multiple alters who manifested distinct dialects and behaviours, including self-harm and disordered eating. Her symptoms were linked to both familial and personal trauma, illustrating early confusion between possession and DID.
Misdiagnosis and Changing Views of Dissociative Identity Disorder ( DID)
Historically, DID was often misinterpreted as possession or hysteria.
- The 19th and early 20th centuries saw DID frequently misclassified under broader labels such as hysteria, a term encompassing various dissociative symptoms. This trend continued even after DID became officially recognized, with cases like Louis Auguste Vivet (1882) illustrating the struggle to fit DID into prevailing diagnostic frameworks.
Modern Recognition
The term “schizophrenia” introduced by Bleuler in 1910 initially encompassed symptoms now associated with DID, contributing to a decline in DID diagnoses. It wasn’t until Ferenczi’s 1932/1949 work that the link between dissociation and childhood abuse was explicitly established, although this insight initially received little attention due to prevailing theories and diagnostic preferences.
Recent Developments
It was not until the recognition of Post-Traumatic Stress Disorder (PTSD) that dissociative disorders, including DID, received renewed focus. Case studies, such as those of Clara Norton Fowler and Chris Sizemore, were crucial in advancing understanding and treatment of DID.
Dissociative Identity Disorder (DID) can develop at any age, but it typically begins in early childhood. While early childhood trauma is often linked to the onset of DID, the disorder can sometimes become more noticeable or be diagnosed later in life.
The misconceptions about Dissociative Identity Disorder (DID)
- Myth: DID is very rare
Fact: DID is not rare; it affects about 1.5% of the population, like conditions like OCD.
2. Myth: People with DID are dangerous or villainous
Fact: Individuals with DID are not more dangerous than the general population and are often more likely to be victims of violence.
3. Myth: DID is not real
Fact: DID is a legitimate condition resulting from severe childhood trauma, not a fabrication or attention-seeking behaviour.
4. Myth: If you have DID, you cannot know you have it.
Fact: People with DID can become aware of their condition and their alters through therapy and self-discovery.
5. Myth: Switches in DID are dramatic and obvious
Fact: Alters do not always make dramatic switches; changes can be subtle and well-concealed.
6. Myth: DID is a disorder of “multiple personalities”
Fact: DID is a trauma disorder characterized by dissociation, not merely a condition of having multiple personalities.
7. Myth: DID happens because the mind shatters under trauma.
Fact: DID results from a failure to integrate into one identity, not from a complete mental break down.
8. Myth: Survivors with DID can switch on demand
Fact: Alters cannot be summoned on demand; external requests do not typically control switching.
9. Myth: Communication with alters is like seeing hallucinations
Fact: Communication with alters usually happens internally, not through external hallucinations.
10. Myth: Parts in a DID system are just variations of the host at different ages
Fact: Alters can be any age, gender, or personality type, not merely reflections of the host’s traumatic experiences.
11. Myth: Because some people lie about DID, all claims are false
Fact: The actions of a few individuals do not invalidate the experiences of those with genuine DID.

12. Myth: People with DID will inevitably cheat or be unfaithful:
Fact: DID does not determine infidelity; individuals with DID are as diverse in their relationships as anyone else.
13. Myth: You can treat DID with medication
Fact: There are no medications specifically for DID; treatment focuses on managing symptoms and addressing the trauma through therapy.
14. Myth: Integration is a must or everyone’s goal in therapy
Fact: Integration into a single identity is not required for everyone with DID; healing can occur with or without integration.
The diagnostic challenges in Dissociative Identity Disorder (DID)
- Inadequate Professional Training: Many mental health professionals have limited training in dissociative disorders. Basic curricula often cover these conditions superficially, leading to a lack of understanding and recognition of DID. This lack of training can perpetuate myths and skepticism about DID’s validity and prevalence.
- Complex Presentations and Comorbidities: DID frequently coexists with other psychiatric conditions such as depression, borderline personality disorder, and psychosis. These comorbidities can obscure the dissociative symptoms and complicate the diagnostic process. Additionally, the symptoms of DID can mimic or overlap with those of other disorders, leading to misdiagnosis.
- Trust Issues: Patients with DID, especially those with a history of trauma, may struggle with trust and fear of being judged. Establishing a therapeutic alliance can be challenging as patients may have fragmented identities that hold different perspectives on the treatment process.
- Unawareness and Avoidance: Many individuals with DID may be unaware of their dissociative states or may avoid acknowledging them due to fear or internal conflicts. This can make it difficult for practitioners to identify and address the disorder effectively. The presence of “covert DID” or partial dissociation adds another layer of complexity to diagnosis.
- Safety and Social Problems: Patients with DID often face significant social and safety issues, including unstable living conditions and toxic relationships. Without a safe and supportive environment, treatment may be less effective, and symptoms may worsen.
Neurobiological Models and Research Of DID
1. Cortico-Limbic Disconnection Model
- This model suggests that DID involves a disconnection between cortical and limbic systems, affecting emotional and self-referential processing.
- Research indicates that DID may be associated with increased activity in the medial prefrontal cortex (mPFC) and reduced activity in the amygdala, which could contribute to emotional numbing and detachment.
2. Structural Brain Abnormalities
Neuroimaging studies have found alterations in brain structure in individuals with DID. For example, variations in grey matter volume and white matter connectivity have been observed, particularly in memory, self-referential processing, and emotion regulation regions.
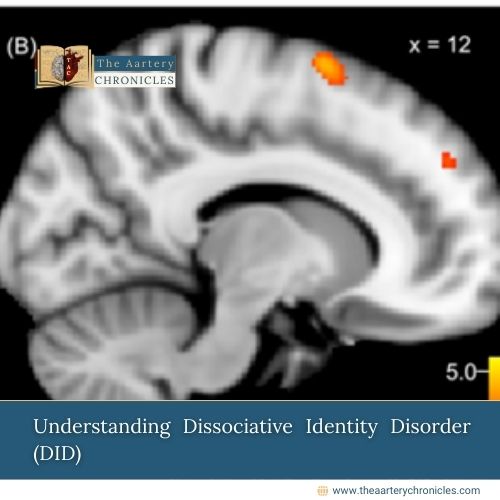
3. Functional Brain Changes
- Functional MRI (fMRI) studies have shown altered brain activity patterns in DID. These include changes in the default mode network (DMN), which is involved in self-referential thought and memory processing.
- Research also highlights differences in brain activity when switching between alters, suggesting distinct neural signatures for different identities or states within DID.
4. Memory Processing and Dissociation
DID is linked to fragmented memory processing, where traumatic memories are compartmentalized. This fragmentation may result from disrupted encoding and retrieval processes in the hippocampus and related structures.
5. Trauma and Neurobiological Impact
DID often develops in response to severe trauma, particularly in childhood. The neurobiological impact of trauma includes altered stress responses and changes in brain areas related to threat processing, such as the thalamus and amygdala.
Conclusion
Understanding Dissociative Identity Disorder (DID) requires a comprehensive approach that encompasses historical context and diagnostic challenges. DID often results from severe trauma, particularly during childhood. The Client’s traumatic experiences and potential emotional abuse may have contributed to her condition. Further diagnostic evaluations and ongoing assessment are necessary to fully understand and address the complexities of the Client’s symptoms and background.
Author
Abhigyan Barooah